
The New York Times Admits Covid Numbers Were Inflated
The official figures were always hopelessly distorted.
A recent New York Times article celebrating “a positive covid milestone” contains a rather remarkable admission. Citing a significant decline in covid deaths, writer David Leonhardt claims that the actual number is almost certainly even lower.
“The official number is probably an exaggeration because it includes some people who had the virus when they died even though it was not the underlying cause of death,” Leonhardt writes.
Leonard mentions this information very casually, as if it were self-evident and not verboten for the vast majority of the pandemic. The claim that official covid numbers were being inflated was repeatedly dismissed as a groundless conspiracy theory. Much of the country, happy to be told what to think instead of taking agency and doing the thinking for oneself, solemnly accepted the figures coming from the CDC and parroted by the mainstream media as evidence that covid was far more deadly than it really is.
So, when Biden announced on May 12 of last year that all American flags at federal buildings were to be flown at half-staff to commemorate one million deaths “from Covid-19,” the national mood was somber, and most people didn’t question the accuracy of the milestone. But the truth — that one million Americans hadn’t died from covid, and that the vast majority died WITH covid — was always accessible for those willing to do a little digging.
With vs. From
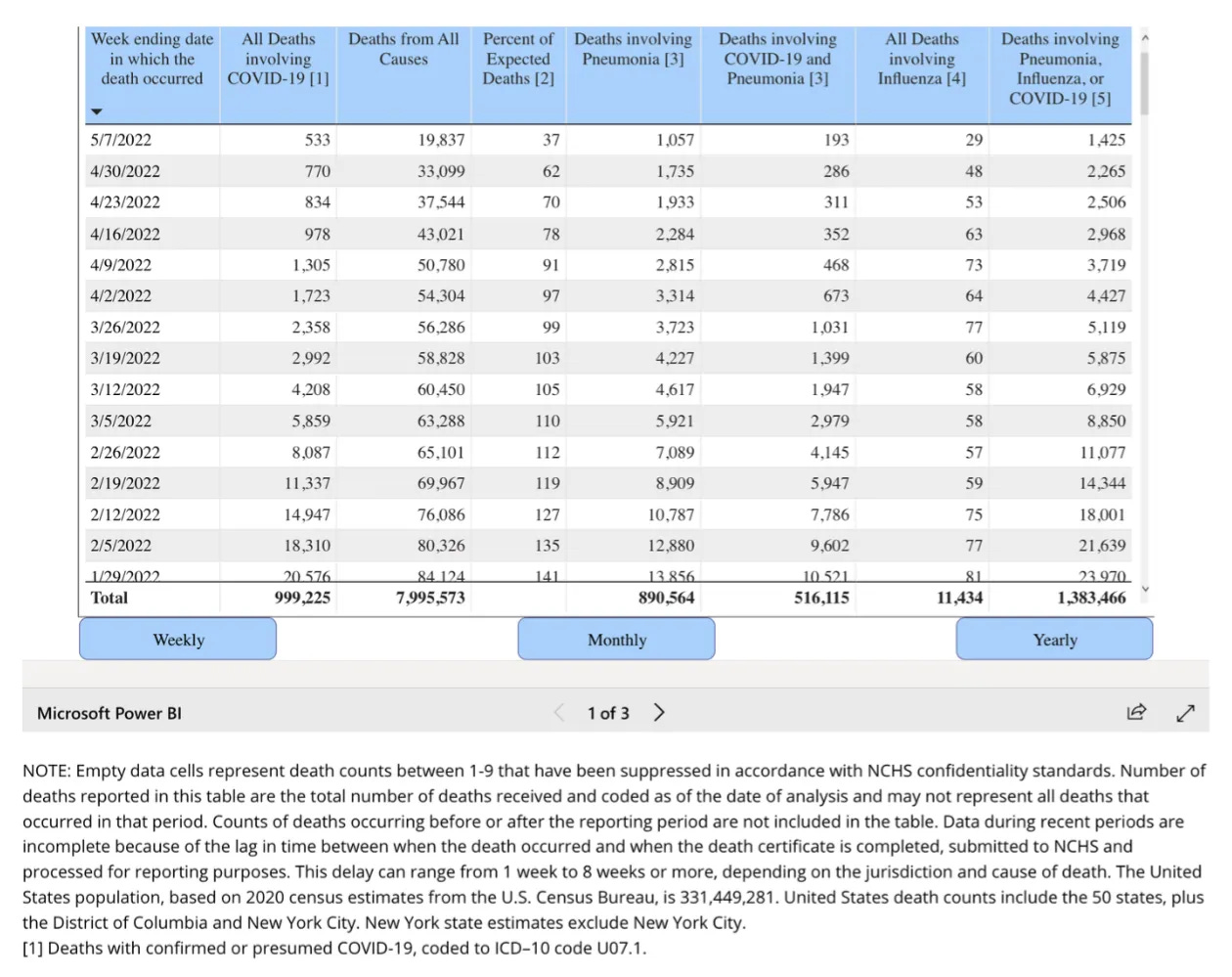
For simplicity’s sake, let’s go back to May 12, 2022 and look at the CDC’s provisional mortality data, which can be seen in the table below, and which just so happens to come with a footnote explaining that “all deaths involving” means “with confirmed or presumed covid-19.” Not “from.”
If you were to look into the CDC’s death certificate reporting guidelines, you’d find that there was no requirement at all that covid be causally responsible to be listed on a death certificate.
Think about that.
Beginning in March 2020, the CDC issued guidance instructing physicians to add covid to death certificates if it were merely assumedto have contributed to the death:
It is important to emphasize that Coronavirus Disease 2019 or COVID-19 should be reported on the death certificate for all decedents where the disease caused or is assumed to have caused or contributed to death. — The National Vital Statistics System
This guidance led public health officials to so broadly define what constitutes a “covid death” that it almost beggars belief. Here, for example, is Illinois’s director of public health talking to reporters in early May 2020:
I just want to be clear in terms of the definition of ‘people dying of Covid.’ The case definition is very simplistic. It means, at the time of death, it was a Covid positive diagnosis. That means, that if you were in hospice and had already been given a few weeks to live, and then you also were found to have Covid, that would be counted as a Covid death. — Dr. Ngozi Ezeke
And here’s the rule stipulated by the Oregon Health Authority:
Deaths in which a patient hospitalized for any reason within 14 days of a positive COVID-19 test result dies in the hospital or within the 60 days following discharge.
In an interview with KGW news about this definition, Oregon Health Authority spokesman Fred Modie was asked a hypothetical: If someone were to die from a motorcycle crash and also had covid, would that be counted as a covid death?
The glossed-over distinction between covid killing someone and someone dying with covid — or even just assumed to have died with covid — should bother you, and all the more so because it followed guidance handed down by the CDC, our nation’s medical luminaries—experts all, to be sure.
Need I point out that the skewed stats distorted the actual risk that covid poses? Take a look at this MMWR:
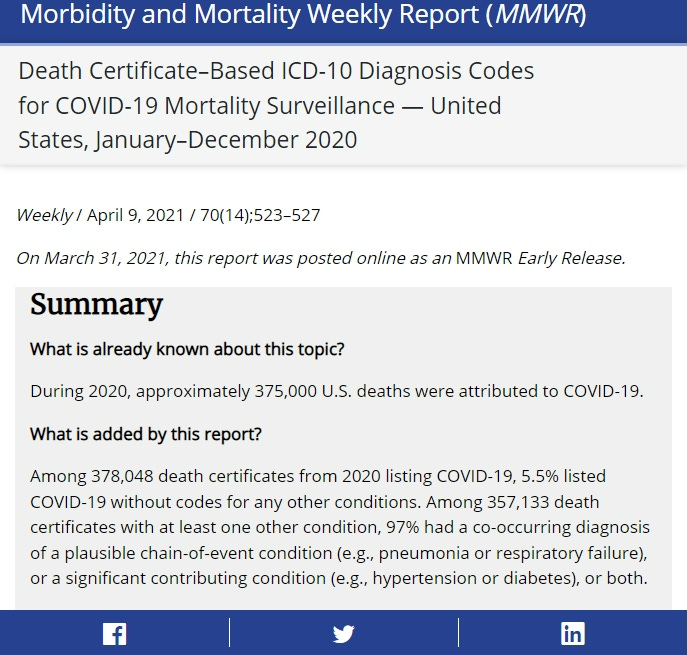
The Head of the Health Emergencies Program at the WHO basically (and accidentally, it would appear) confirmed an infection fatality rate of 0.14%, which is comparable to the flu. But the numbers people were fed based on an over-classification of deaths caused by covid suggested a virus that killed indiscriminately as opposed to one that almost exclusively targets the very old, sick, and obese.
This is usually when some folks revert to anecdotal evidence, pointing to someone they personally knew who died from covid. But that doesn’t mean covid is anywhere remotely as dangerous as the public was led to believe, or that it’s untrue that whichever way you want to philosophically break it down, the costs, both short-term and long, of conflating the danger of a novel coronavirus to such an egregious degree that the most idiotic, authoritarian public health response ever was imposed on society at the expense of everything else were unwarranted.
You can’t even play the “Well, it was only later on that we realized. . .” card.
It was known in March 2020 that, per a major controlled study conducted in France, there was no excess mortality — zero — from this coronavirus compared to other flus. In fact, a comparable Chinese study in February 2020 confirmed the same thing: SARS and MERS were both much more lethal and did not occasion the destruction of the economy, government consolidation of wealth and power in some good old fashioned highway robbery at the expense of everyone outside the elite class, and long-term school closures.
A Casedemic
It gets worse, of course, with regard to the hysteria-inducing numbers used to justify lockdowns and the trampling of civil liberties. The sloppy definition of a covid “case,” combined with how wildly inaccurate our covid tests are, led policy expert Tam Hunt to refer to the pandemic as a “casedemic.” I’m inclined to agree. Consider, for example:
In November of 2020, the FDA warnedthat up to 96% of all covid antigen test positives could be false positives in screening programs at a low 0.1% active disease prevalence. Which you’d think would matter quite a bit, given that we were at or near that level of active disease prevalence for most of the pandemic.
After antigen tests were rolled out widely for weekly or even biweekly screening in the UK, government officials warned in internal email discussions that up to 98% of the antigen test positive results could be false positives because of low active disease prevalence.
In an August 2020 New York Timesarticle, a number of virologists warnedthat the much ballyhooed PCR tests, supposedly the gold standard for covid testing, were being used in such a way that up to 90% of the positive tests were effectively false positives.
All of this and more was ignored. And as if that weren’t bad enough, in an unprecedented move, the CDC defined a “confirmed case” of covid as a positive lab test result only. A “probable case” was even more loosely defined, with not even a test required.
No consideration of symptoms was required for a confirmed or probable case.
In an essay in the San Francisco Chronicle, Dr. Monica Gandhi summed it up nicely:
In the history of epidemiology, experts have never counted individuals without symptoms into these definitions. A ‘case’ was previously defined as a symptomatic person who displayed signs of illness stemming from a pathogen.
In practice, what happened was the complete reliance on positive test results — regardless of symptoms — for cases tallied in public databases.
Uniform case definitions for a number of diseases were first established by the CDC and CSTE in 1990 for obvious reasons. The last time the general criteria were modified was in 1997. The 1997 report states:
These case definitions are to be used for identifying and classifying cases, both of which are often done retrospectively, for national reporting purposes. They should not be used as criteria for public health action.
And so but of course the CDC didn’t follow its own guidance. When the coronavirus came around in 2020, they inexplicably deviated from their own policy. Definitions during the SARS outbreak in 2003 and H1N1 in 2008 required clinical symptoms and laboratory confirmation for a case to be “confirmed.” Even the case definition for the flu requires both clinical and lab evidence for a confirmed case.
But for covid? Nah. A confirmed case required only “confirmatory laboratory evidence.”
Keep in mind all the 24/7 coverage the mainstream media churned out about the spread of covid, their big scary numbers ticking ever-upwards and practically glued to the side of television screens—and always utterly devoid of contextualization. Outlets like the New York Times went out of their way to foment panic and ignore positive news, shaping an alternate reality in which the grim reaper was omnipresent and leading paranoid corona-totalitarians to behave as if the world were one big infectious disease ward.

The change in case definition and the eschewal of symptomatic considerations obviously led to inflated numbers, but the tests themselves are so egregiously inaccurate that the official numbers will forever remain hopelessly wrong. It must be emphasized that this was known by Fauci and his public health minions but never addressed. Stats were allowed to balloon far, far beyond anything resembling the truth.
The false positive paradox is why the “casedemic” misnomer is no more a misnomer than “pandemic” is. When you adopt “surveillance testing” — the widespread testing of people who aren’t showing any symptoms — this practice is proven to result in high numbers of false positives even if the tests you’re using are accurate. But covid tests are NOT accurate, and this led to what Tam Hunt calls “the false positive catastrophe.” The fallibility impacts not just case numbers, which, as mentioned above, are determined simply by tallying positive test results, but also hospitalization and mortality figures since these categories also require nothing more than positive test results.
All of this is compounded even more because, as mentioned in the second bullet point above, when disease prevalence is low — that is, the number of active infections — the vast majority of positives from mass surveillance testing are in fact false. And various studieshave made it abundantly clear that disease prevalence has been low throughout the entire pandemic.
None of this is new, either. Indeed, it was known very early on, and was even mentioned — though very seldomly — by the mainstream media. Harvard epidemiologist Westyn Branch-Elliman wrote about this phenomenon in an article published by U.S. News and World Report, wherein she and her coauthors described how “at the 0.1% or so Covid-19 active infection rate we’re seeing in schools this summer and fall, and a 95% accurate test, we’re likely to see literally 71 out of 72 test positives be false positives.”
71 out of 72.
In sum, the overly-inclusive definitions and death counts used by the public health establishment and propagated by the mainstream media, along with sloppy standards and lax criteria, turned the pandemic into a self-perpetuating shit show the likes of which will go down in the annals of history as easily the most catastrophic public health response ever. It’s through the distance that only time can give that we’ll come to understand the true magnitude of the pathologized-totalitarian science experiment we were subjected to.
Policymakers, public officials, and zero-covid zealots are beginning to intuit this; they know in their heart of hearts that their refusal to allow for basic cost-benefit analysis, to admit uncertainty and mistakes, and the ways they’ve eroded trust in key institutions when that trust was of dire importance—all of this, they know, played a role in upending people’s lives, and in all likelihood they’re desperately hoping that when it comes time to write the history of the pandemic, the Covid Cult will get little more than a footnote or two. It’s up to us to ensure that doesn’t happen.
As detailed by the Discovery Institute's Geoffrey Gilder, in an open letter to German Prime Minister Angela Merkel, epidemiologist Sucharit Bhakti concluded that with the French study, corroborated by findings from a Stanford antibody seroprevalence study in Santa Clara County, “the case for extreme measures collapses like a house of cards.” Bhakti said that since the virus had already spread widely in the general population, efforts to stop further spread were both futile and destructive.




No comments:
Post a Comment