
Why Antiviral Pharmaceuticals Can’t Possibly Work as Claimed
My recent articles focused on the fantasy of the spike protein:
See here: https://anitabaxasmd.substack.com/p/gas-lighting-and-misdirection-with
and here: https://anitabaxasmd.substack.com/p/misleading-criticism-about-the-dangers
I’m following up with this post about the illusion of antiviral pharmaceuticals supposedly stopping the replication of viruses. For one thing, there is no evidence, that viruses exist, see here:
https://anitabaxasmd.substack.com/p/the-questionable-virus-theory
I delved into claims of Pfizer regarding their antiviral drug Nirmatrelvir, better known as Paxlovid™.
On their website for health professionals 1 they write that it works by inhibiting a certain viral protein, Mpro, necessary for a virus to multiply. They claim that “Nirmatrelvir exhibited antiviral activity against SARS-CoV-2 in cell culture studies across the Alpha, Beta, Gamma, Delta, Lambda, Mu, and Omicron variants.”
One of their citations2 says: “The genome of SARS-CoV-2 encodes non-structural proteins [SARS-CoV-2 Mpro (main protease), also known as 3-chymotrypsin-like cysteine protease (CCP or 3CLpro), papain-like protease, and RNA-dependent RNA polymerase (RdRp)], helicase, structural proteins (spike glycoprotein), and accessory proteins. The non-structural proteins play a key role during the virus’s life cycle, and spike glycoprotein is necessary for the interactions of the virus with the host cell receptors during viral entry. The non-structural and structural proteins were recognized as promising targets for the design and development of antiviral agents against SARS and MERS.”
Again, they cite another study3 to support the claim that the Covid Virus encodes for several proteins such as the before mentioned Mpro but also the spike protein and others. The study they cite as evidence claims: “ Using the first available genome sequences, early studies unraveled the genome organization and expression strategy used by coronaviruses and other nidoviruses. These studies were followed by pioneering bioinformatics, biochemical and genetic studies that established or confirmed the essential functions of many of the replicase proteins, thereby laying a road map for the currently ongoing SARS-CoV-2 research. “
Thus they admit that the genome sequence lays at the foundation of claims about the various proteins in and on the supposed virus using BIOINFORMATICS. This means they use genetic sequence from a computer database that were never proven to encode for any virus but came about by taking snippets of genes from a tissue culture containing RNA and DNA from humans and animals and have a computer put them together like a puzzle, adding gene sequences out of thin air, if the found snippets didn’t fit together. This is confirmed by another article4:
Schematic presentation of the genome of the SARS coronavirus
The existence of the Mpro, the targeted protease, is only based on a genome from a computer database. To do determine the structure of Mpro, they took the genetic sequence, created a plasmid and inserted it into E. Coli to produce it, again based on genetic sequence from a computer created genome! 5
The study nr. 3 above then goes on to describe how the virus enters the host cell by the spike protein attaching to ACE receptors, a process and claim I took apart in the above mentioned articles on my Substack.
The study also refers to another study6explaining the mis-nomered isolation process of the virus and the cytopathic effect they take as proof for the presence of a virus, which it is not.
They then describe the process they put the cells from cell cultures through to prepare them for electron microscopy which sounds like a torture chamber for cells:
“Supernatant from human airway epithelial cell cultures that showed cytopathic effects was collected, inactivated with 2% paraformaldehyde for at least 2 hours, and ultracentrifuged to sediment virus particles. The enriched supernatant was negatively stained on film-coated grids for examination. Human airway epithelial cells showing cytopathic effects were collected and fixed with 2% paraformaldehyde–2.5% glutaraldehyde and were then fixed with 1% osmium tetroxide dehydrated with grade ethanol embedded with PON812 resin. Sections (80 nm) were cut from resin block and stained with uranyl acetate and lead citrate, separately. The negative stained grids and ultrathin sections were observed under transmission electron microscopy.”
There is no way images from such cells can give a picture that even remotely resembles a living cell.
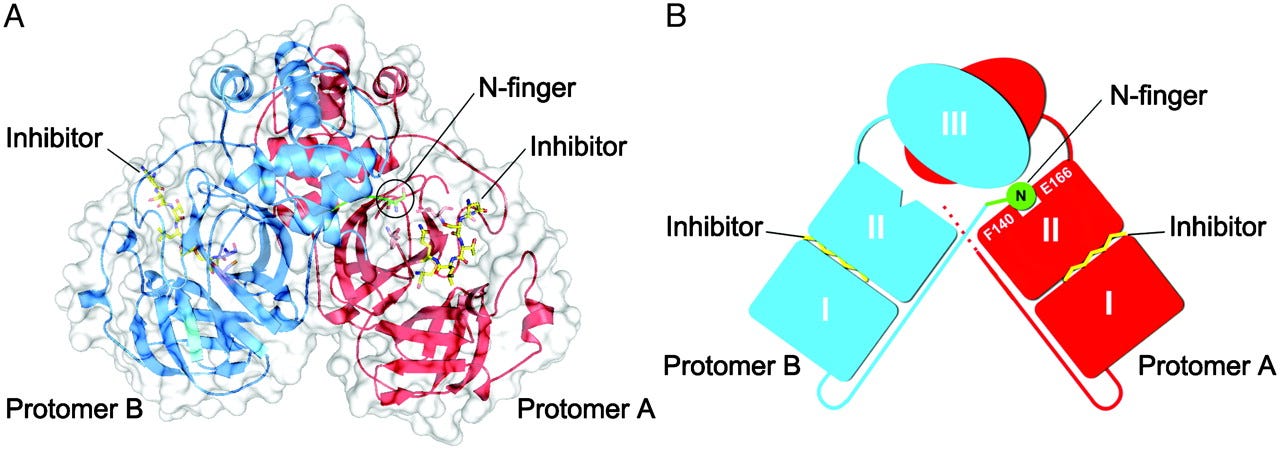
They did Crystallographic studies on the thing they found based on a genetic sequence and ran with it showing all kinds things they found such as:
“SARS-CoV Mpro forms a dimer in the crystal (and in solutions at concentrations of >1 mg/ml) with the two protomers (denoted as ”A” and ”B”) oriented almost at right angles to each other (Fig. 1 A and B), in an arrangement that is similar to the HCoV and TGEV Mprostructures.”
They show impressive computer models how that Mpro protein supposedly looks like, but it’s all built on thin air of a genetic sequence in a computer.
The real effects:
Nirmatrelvir though is an inhibitor of the the P450 cytochrome enzyme family CPY3A4 enzyme the body needs to metabolize and detox pharmaceuticals, besides other things for sure. After all, evolution didn’t have the body make an enzyme to metabolize pharmaceuticals that haven’t been invented yet. When this enzyme is inhibited, toxicity happens that explains the real effects, usually called side effects.
On the website Pfizer lists one study that supposedly proves the effectiveness of their product:
“A total of 2246 patients underwent randomization; 1120 patients received nirmatrelvir plus ritonavir and 1126 received placebo. The incidence of Covid-19–related hospitalization or death by day 28 was lower in the nirmatrelvir group than in the placebo group by 6.32 percentage points”.
They then translate this absolute (measly) risk reduction of 6.32% into 89.1% relative risk reduction which looks better. What we don’t know is how the patients were selected in the placebo group. They say they had the same comorbidities as the verum group, but were theirs just as severe as in the placebo group? Anybody dying within 28 days of a positive “test” result was counted as having died from Covid. What did they actually die of?
What really is astonishing is this statement: “Fewer serious adverse events and adverse events leading to treatment discontinuation occurred with nirmatrelvir plus ritonavir than with placebo.” There is of course such a thing as the nocebo effect in that the mind creates adverse effects in the body usually because these effects are drilled into patients as being possible. Was the placebo group given different information about such effects than the verum group to mess with their minds?
There are quite a few places in a study design that can be fidgeted with to provide the desired outcome. I don’t know the answers to these questions, but the questions need asking.
As you can see, taking apart studies entails diving down into the citations, and then from the study the citation refers to that studies’ citations and down the cascade of several levels it goes to find the truth.
Citations:
1. https://paxlovid.pfizerpro.com/why-paxlovid/mechanism-of-action
2. https://pubs.acs.org/doi/full/10.1021/acscombsci.0c00058#
3. https://www.nature.com/articles/s41580-021-00432-z
4. https://febs.onlinelibrary.wiley.com/doi/full/10.1111/febs.12936
5. https://www.pnas.org/doi/full/10.1073/pnas.1835675100
6. https://www.nejm.org/doi/full/10.1056/nejmoa2001017:




No comments:
Post a Comment